Anatomy of the Volar Distal Radius
David L. Nelson, MD, Jorge Orbay, MD, and Randy Bindra, MD
Last updated June 2, 2008
Purpose: A cadaveric study of the volar distal radius was performed to better understand the anatomy relevant to the volar approach for distal radius fractures.
Methods: Three investigators, separately or collectively, dissected six cadavers and examined nine dried bones. Several anatomic features were identified in each specimen that may be useful to surgeons when placing a volar plate. The findings were confirmed in greater than 200 subsequent surgeries and in many volar plate cadaver workshops.
Results: The following anatomic features were identified and descriptive names were proposed to facilitate discussion: volar radial tuberosity, fibrous transition zone, watershed line, volar radial ridge, pronator quadratus line, and lunate facet buttress.
Conclusions: The presence of six anatomic features was constant
Introduction
The volar approach has become popular for the fixation of distal radius fractures. Our experience with this technique raised questions about details of anatomy and prompted a cadaveric study. The three faculty members of this ICL, both individually and jointly, dissected six cadavers and examined nine dried bones. Several consistent anatomic features were identified that may be useful to surgeons when placing a volar plate. The results have been confirmed in greater than 50 subsequent surgeries and cadaver plating labs. Simple, descriptive names (no eponyms) are proposed to facilitate discussion among surgeons.
Volar Radial Tuberosity
A tuberosity exists on the radial margin of the pronator quadratus fossa (marked "x" in Photograph 1). It can vary from only a millimeter to about 3 mm in size, but it is invariably present. The tuberosity is easily palpable clinically, volar and proximal to the radial styloid. We propose the name "volar radial tuberosity" for this structure.
Clinical Relevance: Plates that are placed too radial will be pronated and not lie flat on the radius. In addition, these plates may be palpable to the patient, requiring subsequent removal.
Volar Radial Ridge
A ridge of varying prominence extends proximally from the volar radial tuberosity and marks the radial limit of the pronator quadratus fossa (represented by the green line in Photograph 1).We propose the name "volar radial ridge" for this structure.
Clinical Relevance: Although not usually in the way of volar plates, the ridge could pronate a plate placed too proximally and radially. To avoid this, some surgeons routinely rongeur the ridge to provide a flat surface. Proper plate placement should avoid the necessity to rongeur the ridge.
Fibrous Transition Zone
There is a distinct and consistent region of adherent fibrous tissue that exists between the distal margin of the pronator quadratus and the mobile volar wrist capsule. The proximal margin of this fibrous tissue does not move with the volar wrist capsule as the wrist is flexed and extended, is firmly attached to the radius over a broad area, and extends further proximally than what would normally be called the origin of the volar wrist capsule. We propose the name "fibrous transition zone" (FTZ) to describe this region, and the name "pronator quadratus line" (PQ line) to describe the linear boundary between the distal margin of the muscle and the proximal extent of the volar fibrous tissue.
Clinical Relevance: Leaving a rim of this fibrous tissue attached to the pronator quadratus will facilitate repair of this muscle. The fascia of the pronator quadratus is so thin that the standard incision and suturing technique does not provide a secure repair, and is more an exercise in imagination than reconstruction. On the other hand, incising the FTZ just distal to the PQ line by two millimeters or so provides a strong edge to the pronator for suture repair and allows a secure closure. This in turn allows the pronator muscle to form a thick and reliable interposition between the distal edge of the plate and overlying flexor tendons. Incidentally, incising the PQ just lightly into the fibrous edge of the first dorsal compartment will also allow a secure closure of the radial border of the pronator quadratus. While the demarcation of the FTZ and the volar wrist capsule is not distinct, we feel that distinguishing the FTZ from the volar capsule is important. We do not believe that dissection of the FTZ causes instability or capsular scarring and stiffness. On the other hand, dissection of the volar capsule proper can cause both instability or scarring of the mobile fibrous tissue of the capsule. In addition, elevation of the FTZ will facilitate visualization of the volar fracture fragments, yet not injure the volar wrist capsular ligaments.
Watershed Line
There is a theoretical line marking the most volar aspect of the volar margin of the radius, which is distal to the PQ line and is covered by the volar capsule (indicated by arrow in Photograph 2). We propose the name "watershed line" for this imaginary line.
Clinical Relevance:
Any hardware placed volar to this line would function as a fulcrum for the flexor tendons, especially in power grip (wrist extension), potentially risking tenosynovitis or rupture. We feel it is important to ensure that the volar plate does not project above this line. Clinically, it does not appear necessary to do so, as small volar rim fragments can be supported by a K-wire technique.
Lunate Facet Buttress
The lunate facet’s volar rim protrudes volarly more than the volar rim scaphoid facet. Proximally, this volar rim is supported by a buttress of a varying size (in Photograph 1, this structure would be where the initials “PQ”are located). We propose the name “lunate facet buttress”for this structure.
Clinical Relevance:
In some patients, the lunate facet buttress is only a millimeter or so higher than the rest of the volar radius, presenting a relatively flat surface for plate placement. In other patients, the buttress can be several millimeters high. It has been our experience that patients with a high lunate facet buttress usually also have a prominent volar radial tuberosity. When this occurs, the volar surface of the radius is not flat, but has a pronounced rolling contour. Flat volar plates do not fit well in these patients, do not support smaller fragments properly, and are more prominent than properly contoured plates. This prominence can be risk tendon irritation and can be more palpable to the patient.�
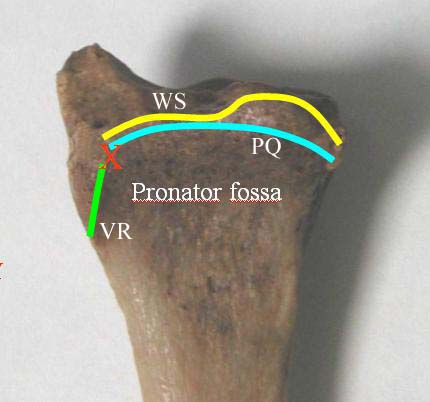
PQ = Pronator Quadratus Line, or PQ Line
WS = Watershed Line,
X = Volar Radial Tuberosity
VR = Volar Radial Ridge

The arrow marks the most volar portion of the radius,
called the Watershed Line
|
