|
|
||||||||||
Synopsis: 75 YO woman, malunion from a radius fx 20 years ago, second fx 8 months ago (Synthes volar plate to the radius and a Synthes 2.0 mm plate to the distal ulna, with suture of TFC complex). At 6 months, full mobility, no pain, but doubts about nonunion on xray. Now, 8 months after her surgery, a third radius fx from a fall. The broken plate was removed and the "fracture site" examined. It appeared to be a synovial nonunion, without evidence for infection. A culture was obtained, to be sure.
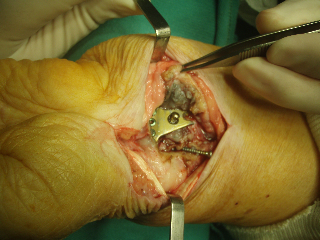
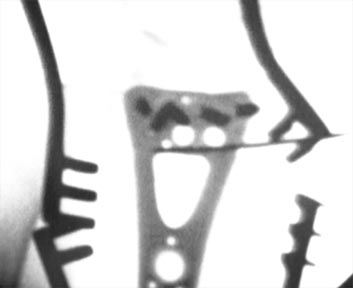
The plate was fractured and a synovial nonunion was apparent.
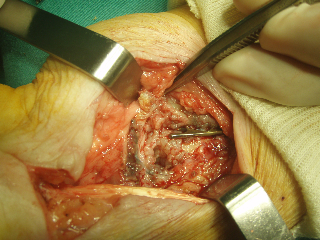
The white, globular material is the synovial nonunion. See below for a magnified view.
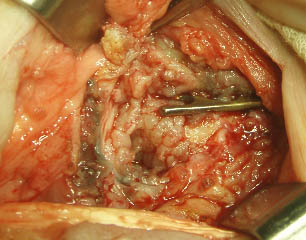
The greatest technical challenge of the surgery was that after complete curettage of the nonunion site, the distal fragment was very small, and there was no volar cortex beneath the plate. (This case well illustrates the fact that the plate takes the place and function of the volar cortex, and the subcondral bone is completely support by the fixed-angle screws.)
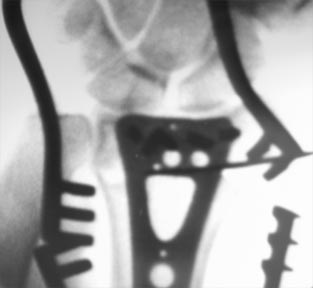
The plate was placed as distally as possible, using facet views to document that none were in the joint. There was a large defect in the metaphyseal region of the radius. Autologous bone graft from the proximal ulna (per the technique of Jorge Orbay) and placed through the triangular hole of the plate. The ulna fixation seemed secure and was left untouched. Patient was placed in a removable orthosis 1
week after surgery. Here is her range of motion at 2 weeks:
Comment by David Nelson, MD, hand surgeon and webmaster of eRadius: The first question is, "Why did she develop a nonunion?" While malunions of the distal radius are unfortunately quite common, nonunions of the distal radius are rare. They are almost always the result of surgical intervention, often involving over-distraction in external fixation. Other causes can be infection, soft-tissue interposition, smoking, diabetes (as in this case), or noncompliance. If the first surgery was well-performed, patient-specific factors need to be addressed (smoking cessation, blood sugar control, and compliance) or the second surgery will have a high risk of nonunion as well. The addition of bone graft and the use of a very strong, very rigid plate should help this fracture to heal. Some technical details: (1) The PA view above is a true PA, and a facet PA would be desirable to document the fact that the screws are out of the joint. You need to look at the lateral to determine the angle that you need to shoot the facet PA; in this case, the distal articular surface is still slightly dorsally tilted. (2) The distal ulnar-most screw has not been documented to be entirely within the bone. The best way to evaluate this is with fluoroscopy while still in the OR. Rotate the forearm until the screw in question is seen absolutely end-on. Often, the titanium plates are just radiotransparent enough that you can see the screw through the plate, because there is a lot more metal in the screw seen end-on than in the plate:
These are two views of the same fluoroscopic image. The left one is the way the image looks normally, the right one is with the contrast turned up. You cannot see the radius anymore, but you can easily see that the top left screw is seen end-on. Referrring back to the normal contrast, you know you are seeing the screw end-on, and therefore you know this screw is entirely within the bone. (3) The shaft screws are a bit short. Note that the lucency of the drilled hole in the dorsal cortex is seen just past the tip of the screws. The quality of the bone in the shaft is normally strong enough to tolerate screw exchange, so I would exchange the screws. When placing them, a nice technique to prevent cross-threading is to turn the new screw backwards (as if removing it), and feel for the slight drop as the threads of the screw align with the threads in the bone, then insert normally. This does not work as well in cancellous bone, and I try very hard to avoid this problem in finger fractures, where screw exchange often results in a loose screw. (4) More importantly, the distal screws are probably a few mm too long. I have learned this the hard way (see Case #12). Work that I have done in the lab shows that you cannot determine, even with fluoroscopy, whether the screw tip is in or out of the bone, and in my own cases, try to place the tip 3 to 4 mm shy of the dorsal cortex. The screw does not get any purchase in the dorsal cortex, and the purpose of the screw is to support the subchondral bone. Overall, however, this patient should heal and be able to resume her activities. |
||||||||||
| About Us | Research | Basic Knowledge | What's New | Forum | Guest Professor | Post a Case | eRadius Conference | Patients | Home |